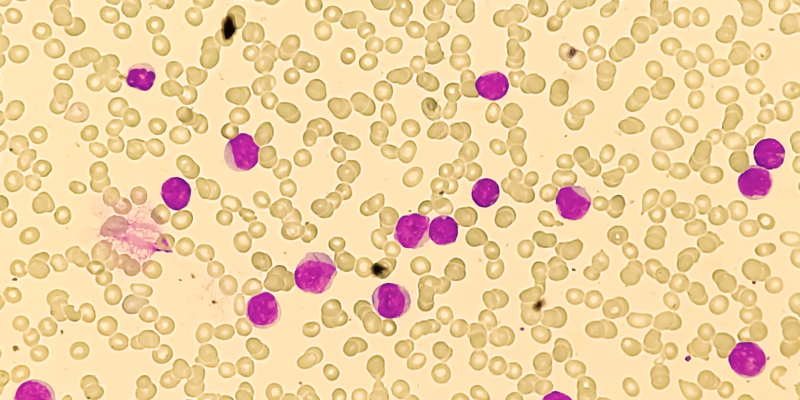
Frontline treatment with decitabine in patients with advanced myeloproliferative chronic myelomonocytic leukemias (CMML) reduced the risk of progression or transformation to acute myeloid leukemia (AML) but did not improve event-free survival (EFS) compared with hydroxyurea, according to results of a randomized phase III trial.
The trial included 170 patients with newly diagnosed, advanced myeloproliferative CMML who were randomized in a 1:1 ratio to receive decitabine (n=84) or hydroxyurea (n=86). Around a third of patients in each treatment group had CMML-2.
Patients received decitabine 20 mg/m2 intravenously for days one through five for a median of five cycles, hydroxyurea 1 g to 4 g daily in 28-day cycles, for a median of six cycles.
The median EFS was 12.1 months in patients receiving decitabine at a median follow-up of 17.5 months, while the median EFS was 10.3 months in patients receiving hydroxyurea (hazard ratio [HR], 0.83; 95% CI, 0.59-1.16; P=.27).
The trial’s primary endpoint was EFS, with events defined as death and AML transformation or progression.
“There was no significant interaction between treatment effect and blast or platelet count, anemia, CMML Prognostic Scoring System, Groupe Francophone des Myelodysplasies, or CMML Prognostic Scoring System–mol risk,” the trial’s investigators wrote.
A significantly higher number of patients (63%) who received decitabine achieved a response than those who received hydroxyurea (35%; P=.0004). However, there was no significant difference in the median overall survival (OS), with a median OS of 18.4 months in patients receiving decitabine and a median OS of 21.9 months in patients receiving hydroxyurea. The median duration of response was 16.3 months in patients receiving decitabine, while it was 17.4 months in patients receiving hydroxyurea.
Decitabine significantly reduced the risk of CMML progression or transformation to AML compared with hydroxyurea cause-specific (HR, 0.62; 95% CI, 0.41-0.94; P=.005). However, this was “at the expense of death without progression or transformation,” the researchers wrote (HR, 1.55; 95% CI, 0.82-2.9; P=.04).
“Compared with [hydroxyurea], frontline treatment with [decitabine] did not improve EFS in patients with advanced myeloproliferative CMML,” the trial’s investigators concluded.
Reference
Itzykson R, Santini V, Thepot S, et al. Decitabine versus hydroxyurea for advanced proliferative chronic myelomonocytic leukemia: results of a randomized phase III trial within the EMSCO network. J Clin Oncol. 2022. doi:10.1200/JCO.22.00437




 © 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.
© 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.