Polycythemia Vera
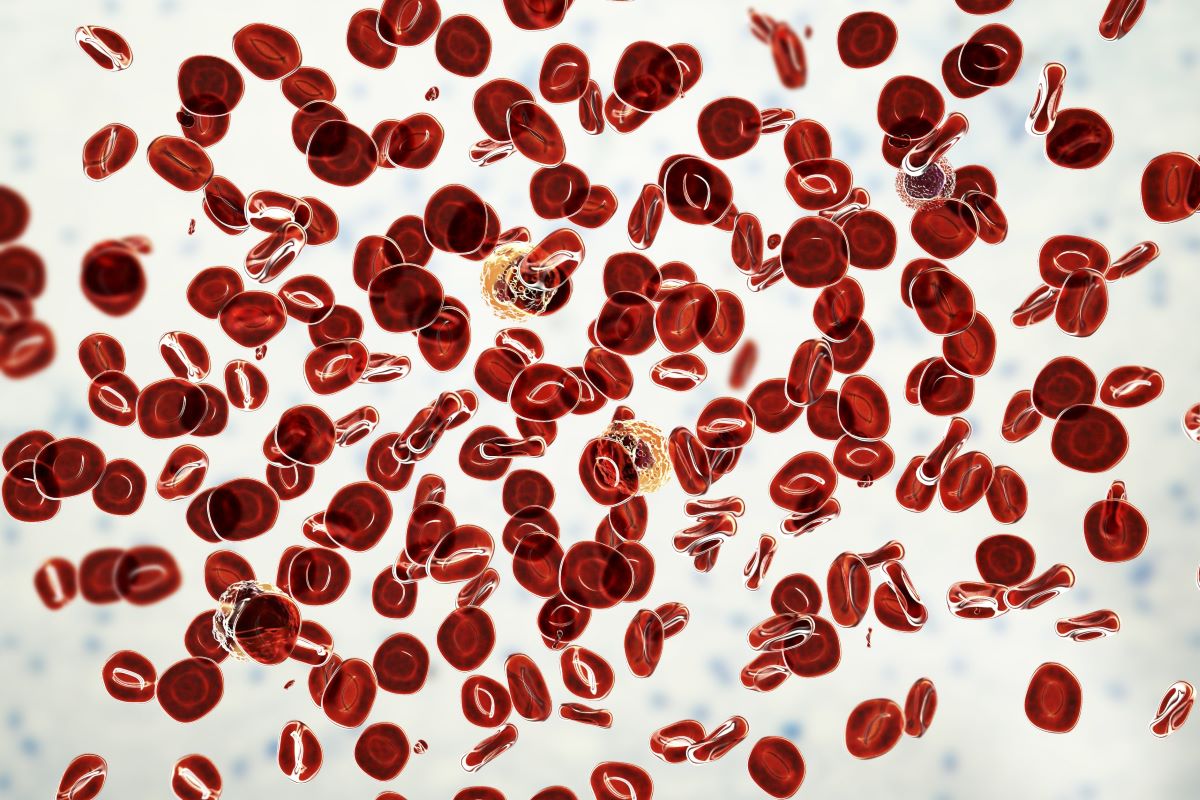
Polycythemia vera (PV) causes an overproduction of blood cells, especially red blood cells, in the bone marrow. This blood cancer is a subset of myeloproliferative neoplasms (MPNs). Treatment of polycythemia vera may include phlebotomy or medication to reduce the red blood cell count.
Advertisement
Advertisement

In a phase 2 trial the hepcidin mimetic increased hematocrit control while reducing phlebotomy and patient-reported symptoms.
A study found limits to the prediction utility of thrombosis history in patients with PV and pulmonary hypertension risk.
A common treatment goal for polcythemia vera is to control HCT with therapy, phlebotomies, and cytoreductive therapies.

VGT-1849A is aJAK2 inhibitor that is designed to have less off-target suppression of JAK1, JAK3, TYK2, and other kinases.

History of thrombotic events, hematocrit ≤0.45 L/L, and JAK2 p.V617F were identified as risk factors for progression.

Myelofibrosis, a rare blood cancer, affects four to six per 100,000 individuals in the United States.

The REVEAL study identified five risk factors, including leukocytosis, duration of time with PV, and more.
Real-world databases lent insight into how often patients with PV experience thromboembolic events.
Knowing who is at high risk in the near term could make it easier to conduct trials of anti-thrombotic therapies.
Developed by Protagonist Therapeutics, rusfertide is a novel injectable synthetic mimetic of the natural hormone hepcidin.
The retrospective study used data on 105 million U.S. patients with linked medical and prescription claims from 2007 to 2019.
Rusfertide quickly induced hematocrit control and maintained improved levels over time in patients with polycythemia vera.
Researchers analyzed PV patients allocated to the ropeginterferon alfa-2b arm of the PROUD-PV/CONTINUATION-PV studies.

CR rates were comparable in both treatment groups, but OS was superior in the ruxolitinib group.

Nearly all myelofibrosis patients are estimated to develop anemia over the course of the disease.

The need for phlebotomies substantially decreased in those who received ruxolitinib after hydroxyurea.

The combined average cost for the index hospitalization and two-year TE-related readmissions was $30,285.

The investigators sought to investigate the diagnostic landscape of polycythemia vera in LMICs.
Researchers presented data from the randomized withdrawal phase of the study at the SOHO Annual Meeting.

From Houston, Texas, to Beirut, Lebanon, the SOHO global community continues to grow thanks to its Ambassador Program.

Dr. Harrison discusses survey results from the LANDMARK survey in patients with polycythemia vera and their physicians.

Just under half (43%) of patients receiving ruxolitinib achieved a CR, while 26% achieved a CR on the best available therapy.

The trial included patients with PV who had at least three therapeutic phlebotomies in the 28 weeks prior to enrollment.

Dr. Kuykendall and colleagues presented their findings during the 2023 European Hematology Association Congress.

Dr. Krecak presented the research during the 2023 EHA Congress.
The main aim of treatment is preventing thrombotic complications.

The FDA could not approve the application in its current form and identified additional requirements for approval.
Hematocrit control was “suboptimal” in more than half of patients with high-risk polycythemia vera.

Srdan Verstovsek, MD, discusses using machine learning to predict resistance to hydroxyurea therapy in polycythemia vera.

Patients with MPN have a high risk of death from cardiovascular causes.
Srdan Verstovsek, MD, discusses the phase III VERIFY trial of rusfertide in patients with polycythemia vera.
Whole blood mutation allele frequency had only weak prognostic value in certain patients with polycythemia vera.
The combination of interferon and ruxolitinib may be a treatment option for newly diagnosed polycythemia vera.
New data support the use of ropeginterferon alfa-2b therapy in patients with low-risk or high-risk PV,
IFNα2 treatment may help reduce the risk of arterial and venous thrombosis in patients with myeloproliferative neoplasms ...
VERIFY, a phase III trial of the hepcidin mimetic rusfertide (PTG-300), is now enrolling patients with PV.
Long-term results from the RESPONSE-2 trial confirm efficacy of ruxolitinib for PV.

In patients with high-risk essential thrombocythemia and polycythemia vera, both hydroxyurea and pegylated interferon-α.
REVEAL is the largest prospective and contemporary cohort of patients with PV in the United States.
Blood Cancers Today delivers the latest news, education, and information relevant to hematologic oncology patients and practices.
Sign up to receive Blood Cancers Today eNewsletters:
 © 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.
© 2025 Mashup Media, LLC, a Formedics Property. All Rights Reserved.